 Nipples are NOT suppose to hurt.
I recently had a client call me in desperation. She said she wanted to breastfeed and knew it was suppose to hurt but she didn’t think she could take it anymore! My response, “Whoa, who said it was SUPPOSE to hurt?” Her mother told her breastfeeding will hurt and she should be “toughening” up her nipples by rubbing them between feeds, preferably with a rough towel. No wonder this poor woman’s nipples hurt! Breastfeeding should not be hurting. If nipples are raw, cracked or bleeding there is a latch problem that needs to be assessed and fixed. Sure, in the first few days the areola may be tender since this area is not use to so much action. However, the pain should not be “toe curling” even to latch. By adjusting position and using latch techniques to encourage a deeper latch, the baby should be able to get on the breast without causing pain. There is no reason you should be “toughening” up your nipples. And please don’t rub them with anything! Some women notice drying in the third trimester, whereas some notice the nipples are suppler than they every have been. If drying happens, applying olive oil as a natural lubricant, or using a commercial nipple cream should help to relieve the dry skin. Avoid washing nipples with soap. Soap washes away natural oils and promotes cracking. Have an IBCLC (Lactation Consultant) assess the damage, or preventatively, have a prenatal consult to have nipples assessed, discuss latch techniques and different positions for breastfeeding and to prepare you for what to expect in the first 72 hours of breastfeeding. Some women have flat, inverted or dimpled nipples that may need assessment and altered breastfeeding positions may be required. Nipple shields and breast shells need to be used with caution. Please note that if you are recommended to use these products, you require close monitoring for milk transfer and milk production. These products can down regulate milk production. Breastfeeding is a natural process and not one that is supposed to invoke pain! Please don’t suffer and please don’t follow old wives tales to “toughen” up a delicate part of your body. If there is pain, call for help. Feeding your baby should be a pleasure and a great bonding experience, not something you dread.
1 Comment
After delivery, a woman's body is recovering from the "Boston Marathon" of birth! Adrenalin starts to ebb and muscles are tired and sore. The uterus continues to contract as it works to get back to it's pre-natal size. What happens when the uterus stages a sit-in? Well, it's not pretty! Post partum hemorrhage causes excessive blood loss either during delivery or immediately after. But what does that have to do with milk production? Let's take a look. The pituitary gland is responsible for secreting prolactin and oxytocin, two hormones essential for milk production and milk ejection. After post partum hemorrhage, the pituitary gland goes into shock and for a short time does not perform its regular duty. 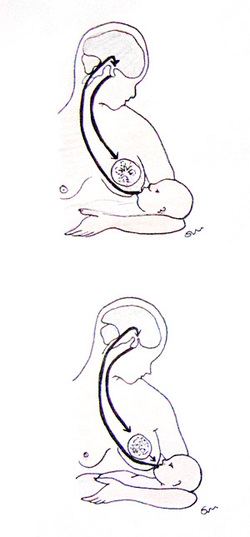 The Prolactin Reflex 1. (Long arrow) Nerve impulses from sucking go to brain 2. (Short arrow) The pituitary gland releases prolactin into the blood 3. (Breast) This causes the alveolar cells to secrete milk and swells the alveoli The Milk Ejection Reflex 1. (Long arrow) Nerve impulses from sucking go to the brain 2. (Short arow) The pituitary gland releases oxytocin into the bloodstream 3. (Breast) This causes muscles around the alveoli in the breast to squeeze milk to the nipple As a result of pituitary dysfunction, prolactin and oxytocin levels are low and consequently, milk production is as well. It is important that mom feed or pump frequently to stimulate the prolactin and oxytocin frequently. After post partum hemorrhage, it is common to have delayed milk production for 4-6 days and insufficient milk supply for as much as two weeks or more. Mom and babe require close follow-up to ensure milk production and weight gain. For more information on post partum hemorrhage or breastfeeding concerns, contact The Breast Start. Picture and information reprinted from http://www.thebreastway.com/index.php/how-it-all-works-breastology/physiology-of-breast-feeding-and-milk-let-down
Babies are born with the innate ability to suck. Newborns suck for more than just satisfying hunger. Sucking is pleasurable, calming and is a pain control mechanisms for babies.
After a baby is born, their bellies are full of amniotic fluid that is swallowed continuously while in the womb. This is why for the first twenty four hours they do not feel hunger. The best time to introduce the breast is within the first hour after delivery. Sucking at breast calms her and reassures her in a world that is not known to her. After she is born an infant enters the active alert stage of wakefulness and this time is important to use as practice for latching and feeding the baby. Over the next twelve hours, newborns enter the “sleepy phase”. It’s often difficult to wake the baby at this stage as she recovers from delivery. Skin-to-skin during this time assists in maintaining her body temperature and stabilizing her heart rate. It’s also the perfect opportunity to allow her free access to the breast. After 12-24 hours, the baby begins to get hungry as the belly empties. Cues that baby is wanting to feed or suck include: · Smacking the lips and tongue thrust movements · Bringing hands to mouth · Head to the side with wide open mouth Crying is a late sign of hunger and it is often difficult to latch her when she has reached this point. Being aware of your baby’s hunger cues is important so she does not get frustrated and she can begin to trust that food will be supplied. Moms often ask why babies suck all the time. Remember that sucking is not just a response to hunger. She may suck to relieve tummy pain, to feel close to mom, to fall asleep. As a response to the frequent sucking, moms often state they “do not have enough milk”. This is common perception occurs because we were not born with volume windows on our breasts! Mom will make milk (supply) as a response to the baby’s sucking (demand). With breastfeeding, demand must occur before supply happens! This is why free access to the breast in the first few weeks is the best way to support your milk supply. The more the baby sucks, the more the breasts are stimulated to make the milk the baby needs, especially after the first few days when the baby will have lost weight. Weight loss is normal in newborns as the body transitions to the extra-uterine world. With good feeding, the baby should regain her birth weight in the first two weeks. The use of pacifiers when breastfeeding is not recommended until mom and dad can be reassured that baby is not hungry. The basic rule of breastfeeding is: if the baby wants to suck, let her do so on mom so that milk production is regulated to her needs. Pacifiers in the first few weeks alter the supply of milk in mom because the baby is not “demanding” that mom supply the milk. In some babies, pacifiers can also alter their suck pattern and interfere with a good latch causing mom pain and discomfort. In situations where mom and baby are separated, it is important to support mom’s milk supply with the use of a breast pump or hand expression. The demand still needs to occur if baby is not present to stimulate the milk production and support the supply. Double pumping is preferred over single pumping because it increases the hormones in mom’s body that are responsible for milk production. It also saves precious time! If milk cannot be used right away, it can be stored for later use. Milk supply normalizes in the first two to three weeks. The breastfeeding rule of thumb is: if baby wants to suck (demand), allow her to do so at breast to assist and maintain the milk production (supply). As you and your baby get to know one another, it will get easier to distinguish her needs and you will become confident that your body is making the necessary supply. For further information on breastfeeding, visit www.thebreaststart.ca |
DaphneDaphne is an RPN, IBCLC and Director of Precious Moments Babeez Dufferin KW Archives
April 2013
Categories |

-
Home
- Contact Us
-
Belleez & Babeez Blog
>
- By Debbie Fazio: Parenting Coach
- Jessica Jhaj PNSW Blog
- By Sabrina: A sleep consultants journey with her new baby!
- By PNSW Ange - It all started with green poop!
- By IBCLC Daphne: The world of breastfeeding
- By Lauren: Sleep training from a moms view
- Guest Blogs:Everything mommy, family & business
- Send us your Blog
- Community Links >
- Meet the Babeez Team
-
Our Services
- Become an Affiliate
- Testimonial Submission
- Join Our Team
- Parenting Video Library
- Privacy Policy
- Make a Donation
- Start a Babeez Franchise
 RSS Feed
RSS Feed